Building Demand for Development
July 13, 2026 Leave a comment
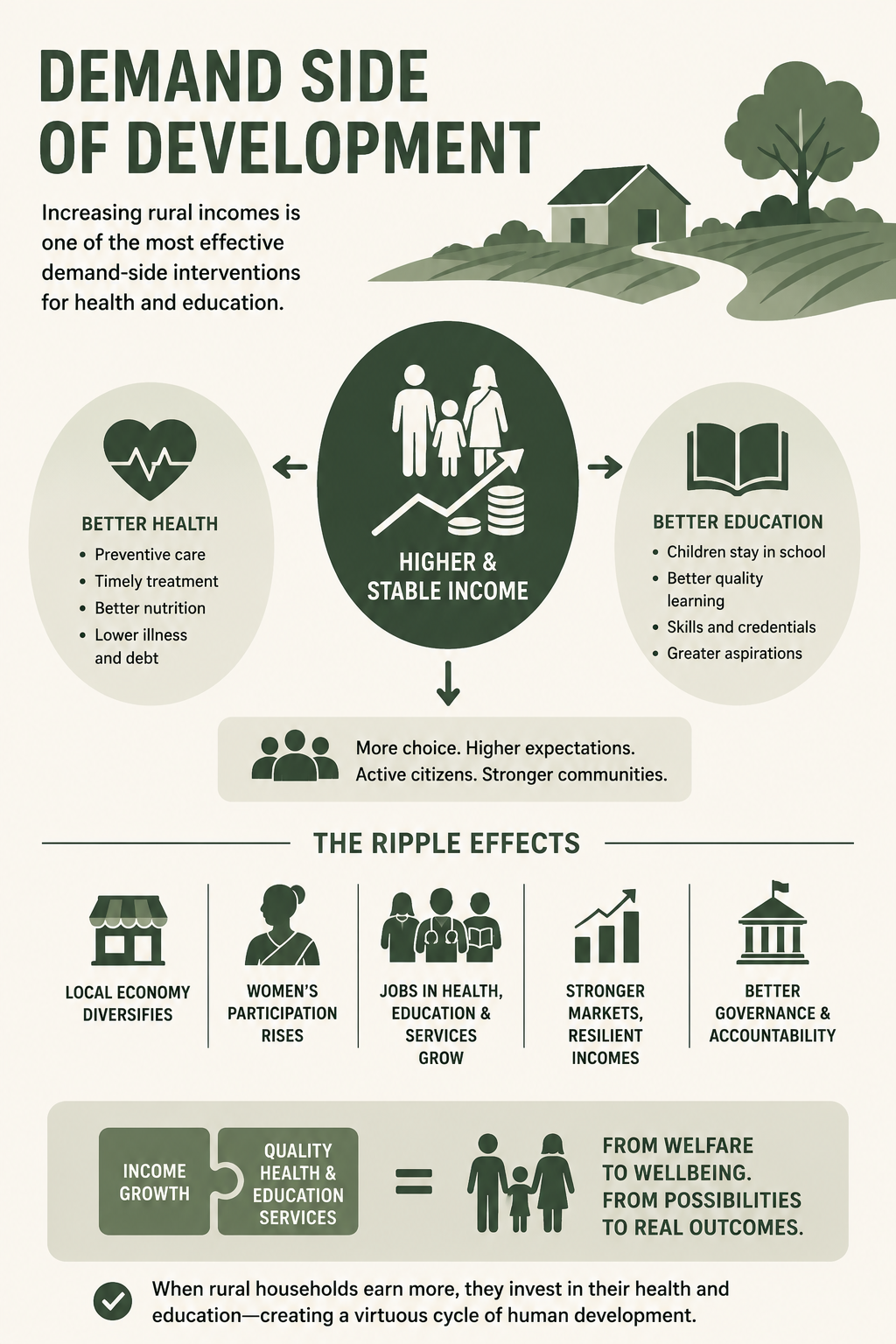
India’s rural development dialogues have treated health, education, and income as parallel priorities often pursued through separate policy silos. Budgets are allocated, schemes are launched, infrastructure is built, and targets are set, all with good intent. However, one foundational truth remains insufficiently acknowledged, that increasing rural incomes is not merely an economic goal but one of the most effective demand-side interventions for health and education. Without income security, even the best school education systems and local health facilities struggle to translate access into outcomes. With income growth, aspirations gain purchasing power, the choice basket expands, and human development accelerates in ways no standalone welfare programme can achieve.
The constraint on health and education in rural India is rarely a lack of awareness alone. Most families understand the value of a healthy body and an educated child, but they cannot act on that understanding consistently. Irregular incomes, seasonal employment, debt cycles, and exposure to shocks force households into a constant state of prioritising needs and what is immediately affordable. In such conditions, preventive healthcare is postponed until illness becomes unavoidable, and education becomes negotiable once opportunity costs rise. When incomes increase, particularly when they become predictable rather than sporadic, this calculus begins to shift fundamentally. I have witnessed this change countless times among the families from rural livelihood and entrepreneurship development programs across multiple states of India, from the north to the northeast.
The first visible change that accompanies rising rural income is in health-seeking behaviour. As disposable income grows, households move from reactive to preventive care. They begin to spend on nutritious food intake, diagnostics, maternal health, and timely treatment rather than relying solely on home remedies or last-resort interventions. This is observable across rural belts where livelihoods have stabilised through dairy cooperatives, non-farm employment, or entrepreneurship opportunities. Increased income reduces the psychological cost of seeking care. A doctor’s visit no longer feels like a financial gamble, and medicine is no longer a choice between recovery and indebtedness. Over time, this shift translates into lower morbidity, higher productivity, and a virtuous cycle of income and wellbeing.
Education follows a similar but slightly delayed trajectory. At very low-income levels, schooling competes with survival. Children’s labour, whether on farms, in family enterprises, or in caregiving roles, has immediate economic value. As incomes rise, the opportunity cost of schooling declines. Families are more willing to keep children in school, invest in better quality institutions, often private schools in their own villages or neighbouring towns, and support supplementary learning such as tuition or digital tools. Crucially, income growth often changes learning outcomes and ambition, and not just enrolment. Education stops being about literacy alone and starts being about mobility, including English proficiency, technical skills, credentials, and pathways beyond the village economy.
This transition from survival to investment is critical as human capital investments respond strongly to income thresholds. Below a certain level of income, households simply cannot afford to plan long-term, and above that critical level, behaviour changes rapidly. Rural India today stands at precisely this inflection point. Decades of infrastructure expansion, electrification, and digital penetration have laid the groundwork. What remains uneven is sustainable income enhancement pathways at scale. Where it happens, demand for health and education services rises organically, often faster than supply systems can respond.
However, increased income alters expectations and does not merely increase consumption. Rural households with higher incomes begin to demand quality, accountability, and outcomes. They compare schools, question teaching standards, seek second medical opinions, and are willing to pay for reliability with profound implications. It challenges the assumption that rural citizens will accept poor service quality indefinitely. It also creates space for private, social, and hybrid service models like low-cost clinics, diagnostic centres, skill academies, and ed-tech platforms that were previously unviable due to weak demand. Income growth can enable choice for households, who would increasingly adopt mixed strategies of using public facilities for some services and private providers for others. This duality can, if managed well, improve overall system performance.
The ripple effects of income-driven demand can extend beyond individual households. As spending on health and education will increase, local economies will diversify. Teachers, health workers, lab technicians, transport providers, and service support staff will find employment closer to home. Women’s participation in the workforce will rise as care responsibilities will reduce and aspirations will expand. These multiplier effects will strengthen rural markets, making income growth more resilient and less dependent on a single sector like agriculture.
However, income growth alone is not sufficient, as demand without supply will lead to frustration, not development. In many rural areas, rising incomes have resulted in out-migration for services, with families travelling long distances or relocating temporarily to access quality healthcare and education. This is not a failure of income-led development, but a failure to anticipate and respond to it. Both public and private supply systems must be designed to scale alongside income growth. Physical access, skilled personnel, digital connectivity, and trust are essential if local ecosystems are to capture the benefits of rising demand.
Livelihood programmes and social sector investments are often conceived independently. Income-generation schemes focus on outputs like jobs created and enterprises supported, while health and education programmes focus on inputs like schools built, staff hired, and beneficiaries enrolled. What is missing is an integrated demand-supply lens. Rural income enhancement should be explicitly recognised as a human development strategy, with parallel investments planned in service delivery capacity. When livelihoods improve in a region, health and education infrastructure should be strengthened proactively, not reactively.
For corporate social responsibility (CSR) and philanthropy, this insight could be particularly valuable. Rather than choosing between livelihoods and social services, funders should see them as sequential and reinforcing investments. Supporting rural entrepreneurship, value chains, or digital livelihoods creates the conditions for sustained demand for health and education. Complementing this with investments in service quality of teacher training, primary healthcare strengthening, telemedicine, or skill education will maximise impact. Fragmented interventions will yield fragmented outcomes, while integrated strategies can create lasting change.
When rural citizens earn more, they become more vocal stakeholders in the local political economy. They demand better governance, transparency, and responsiveness. Health and education, being highly visible services, often become focal points of this demand. Income growth thus strengthens democratic accountability. It shifts the relationship between the state and citizens from charity to entitlement, from gratitude to expectation.
India’s development journey offers ample evidence of this dynamic. States like Gujarat, Tamil Nadu, and Maharashtra that have successfully diversified rural incomes through improved irrigation, manufacturing clusters, or services consistently outperform others on health and education indicators. The lesson is that the effectiveness of social spending is amplified when households have the means to engage with it meaningfully. Supply creates possibility, and income creates participation.
As India looks ahead to the next phase of rural transformation, the question is no longer whether to invest in health, education, or livelihoods, but how to sequence and integrate them. Treating income growth as the foundation of demand generation reframes the debate. It reminds us that people are not passive recipients of services, but active decision-makers whose choices shape outcomes. Empowering those choices through income security may be the most humane and pragmatic development strategy to have. This has the potential of unlocking a chain reaction that will turn latent needs into effective demand, services into systems, and welfare into wellbeing. Healthier bodies and educated minds do not emerge in isolation, but they grow where households have the freedom to choose them. And that freedom, in rural India, begins with income.
If this essay made you reflect on how income shapes opportunity, choice, and human potential, subscribe to my blog for one new article every week in your inbox. It’s free!
(Disclaimer: The opinions expressed are those of the author and do not purport to reflect the views or opinions of any organisation, foundation, CSR, non-profit or others.)
The cover image is generated using AI

